

Book Your Appointment Today!
Our staff will reach out to you shortly
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.

You’re sitting in an orthodontic consult, expecting to hear about braces or clear aligners. Then the orthodontist says a phrase that makes your stomach drop: “We may need to remove a tooth.”
That reaction is normal. Individuals often hear “extraction” and immediately think pain, gaps, a changed face, or a treatment plan that suddenly feels more serious than they expected. Parents often worry they’re agreeing to something too aggressive. Adults often wonder if there’s another way.
The good news is that an orthodontist tooth extraction isn’t a default move. It’s a specific tool for a specific problem. When it’s recommended, the goal is usually simple: create the right amount of space so teeth can move into healthier positions without forcing them outside the limits of the jawbone or leaving the bite unstable.
A careful treatment plan should never feel like a sales pitch or a mystery. It should feel like a conversation. If you want a helpful framework for those conversations, this guide to shared decision making explains how patients and clinicians can weigh options together, ask better questions, and choose a plan with confidence.
If you’ve been told an extraction might be part of orthodontic treatment, clarity matters more than reassurance alone. You need to know why it might help, who does it, what recovery is like, what alternatives exist, and how to think about cost without panic.
A common scene goes like this. A teen comes in because the front teeth are crowded and one canine is erupting in the wrong place. Or an adult wants aligners but has lips that feel “pushed forward” and teeth that don’t fit neatly in the arch. The orthodontist studies the X-rays, photographs, and bite, then says extraction may give the best result.
That moment can feel heavy because “pulling a healthy tooth” sounds backwards. Patients often ask, “Why not just straighten what’s already there?” That question makes sense. Teeth are not books on a shelf that can always slide over if you push hard enough. They sit in bone, and that bone has limits.
Sometimes the kindest plan is not the one that avoids every intervention. It’s the one that creates enough room for teeth to move safely and stay stable.
People also get confused because they’ve heard opposite messages online. One post says extractions are outdated. Another says they solve everything. Neither extreme is helpful. Orthodontics is more like tailoring than following a recipe. Two mouths can look similar at first glance and still need different plans.
Three questions usually matter most at this stage:
If you’re in this spot right now, pause before assuming extraction is either obviously right or obviously wrong. Ask to see the problem on your scans and models. Ask what happens if you don’t remove teeth. Ask what tradeoffs come with each option. Those questions usually turn fear into something more useful: understanding.
Think of your dental arch like a room with fixed walls. If too many chairs are crammed into that room, you can’t arrange them neatly just by shoving harder. You either need to make the room bigger, reduce the size of what’s inside, or remove a few items so everything fits correctly. Orthodontic extraction works on that same principle. It creates room when the teeth and jaws don’t match well enough for a healthy alignment.

The most direct reason for extraction is crowding. If the arches are too small for the size and position of the teeth, lining them up without making space can push teeth outward, strain gum support, or leave the result unstable.
Researchers reviewing orthodontic treatment patterns found that over a 32-year period, extraction frequency decreased from 61.1% to 40.8%, yet 45.8% of patients in a large study still required extractions, most often in cases involving significant crowding and Class II malocclusions. You can read that analysis in this orthodontic extraction trend study.
Patients often think extractions are only about “making room for crooked teeth.” Sometimes they’re also about correcting how the upper and lower teeth fit together. If the front teeth are too far forward, if the overjet is pronounced, or if one bite pattern makes the smile look and function unbalanced, removing selected teeth can give the orthodontist room to bring everything into a healthier relationship.
That’s why extraction decisions can’t be based on selfies or quick impressions. The bite matters. Jaw relationship matters. Where the roots will end up matters.
This part gets emotional fast because people worry about looking sunken or older. The primary goal of a well-planned extraction case is the opposite. The orthodontist is trying to place the teeth where they support the lips and profile appropriately for that individual face.
Practical rule: Extraction is not the goal. A healthy bite, stable alignment, and balanced facial support are the goals.
Here’s a simple way to think about it:
| Situation | What the orthodontist is trying to solve |
|---|---|
| Teeth overlap heavily | Create enough room for alignment |
| Front teeth protrude | Reduce strain on the lips and improve bite position |
| Bite is mismatched | Coordinate upper and lower arches more precisely |
The important takeaway is that extractions are less common than they used to be, but they’re still part of modern orthodontics because some mouths need actual space, not wishful thinking.
The orthodontist is usually the professional who decides whether an extraction belongs in the treatment plan. That doesn’t always mean the orthodontist is the one who physically removes the tooth. In many cases, another dentist performs the extraction based on the orthodontic plan.
People get confused. They hear one office recommend extractions, then they’re referred elsewhere, and suddenly it feels like too many handoffs. The easiest way to understand it is to separate planning from procedure.
The orthodontist studies the bite, tooth positions, root angulation, facial profile, and how the spaces will later be closed. That planning step is critical because the wrong tooth removed at the wrong time can complicate treatment.
This matters even more in less typical cases. As described in this review of asymmetrical extraction protocols, some plans use a single lower premolar or three premolars instead of the more familiar two or four. Those strategies can help with midline deviations and certain bite relationships, but they require precise diagnosis and strong coordination between orthodontic and restorative thinking.
A general dentist often handles routine extractions, especially when the tooth is fully erupted and access is straightforward. Many patients are surprised by this, but it’s common. If the tooth is healthy, visible, and in a position that allows safe removal, a general dentist may be the right person.
An oral surgeon usually steps in when the case is more complex. That can include impacted teeth, unusual root shapes, difficult access, heavy anxiety that may call for deeper sedation, or cases where anatomy raises the surgical difficulty.
Here’s a simple comparison:
The best experience usually comes from clean communication. Everyone should agree on which tooth is coming out, why it’s that tooth, and when orthodontic movement begins afterward.
If your case involves braces, aligners, crowding, and possible restorative work later, ask one practical question: “Who is coordinating the whole sequence?” That question often tells you how smooth the process will feel.
Most patients fear the unknown more than the extraction itself. Once you understand the steps, the process usually feels much more manageable.

The visit usually starts with confirmation of the treatment plan, updated imaging, and a review of your medical history. Many modern practices use digital AI-powered X-rays to help identify root shape, tooth position, and nearby anatomy with more precision. That planning reduces surprises.
You should also expect a conversation about comfort. Some patients do well with local anesthetic alone. Others need additional support because they’re anxious, have had difficult dental visits before, or are facing a more involved procedure.
Before the day ends, you should understand:
The key point is this: you should feel pressure, not sharp pain. After the area is numbed, the dentist loosens the tooth and removes it in a controlled way. For a simple orthodontic premolar extraction, the visit is often shorter and gentler than patients expect.
Many people worry that “pulling a tooth” means force and trauma. In reality, the goal is the opposite. The clinician uses technique, mechanical advantage, and careful tissue handling to protect the surrounding bone and gums because those tissues matter for later orthodontic movement.
There’s a real anatomical reason some extractions feel easier than others. According to this clinical review of maxillary and mandibular extraction anatomy, the maxilla, or upper jaw, has softer and more vascular bone than the mandible, or lower jaw. That means upper extractions are often quicker, local anesthetic tends to penetrate well, and healing is often faster and more predictable.
Patients notice this in practical ways. An upper premolar removed for orthodontics may settle down more quickly. A lower extraction can feel denser or sorer because the bone is typically thicker and less forgiving.
Recovery mindset: Expect improvement day by day, not hour by hour.
A short visual overview can help if you like seeing the process explained before your appointment.
The first day is mostly about protecting the blood clot and keeping inflammation under control. Soft foods, rest, and careful hygiene make a big difference.
A practical checklist:
If you want a more detailed day-by-day overview, this tooth extraction recovery guide is a useful follow-up resource.
Recovery is usually easier when you know what’s normal. Mild soreness, tenderness, and some limited chewing on that side are expected. Feeling blindsided is what makes it harder.
Many patients ask the same question right away: “Can we do this without removing teeth?” Sometimes yes. Sometimes no. The right answer depends on how much space is needed, where that space is needed, what the bite is doing, and what changes would be acceptable to the face and gums.
Before comparing alternatives, it helps to address the biggest fear directly. Patients often worry that extraction will hollow the face or ruin the profile. That concern is understandable, but facial change in orthodontics is usually more measured than online stories make it sound.
According to this discussion of premolar extraction and profile change, 1 mm of incisor retraction typically changes lip position by about 0.6 to 0.7 mm. That doesn’t mean profile changes never matter. It means they should be discussed realistically, with planning based on your own anatomy rather than internet extremes.
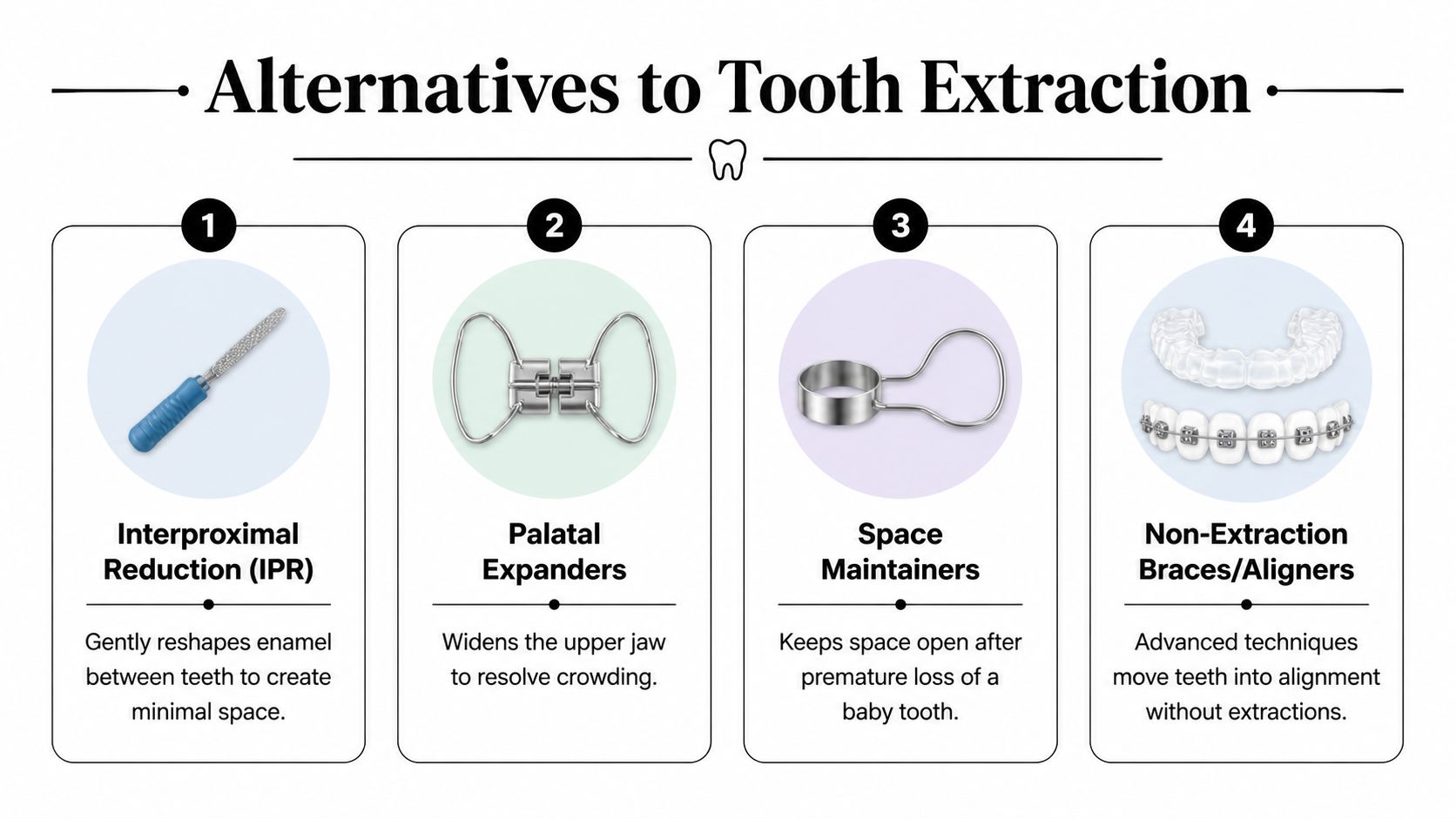
A strong non-extraction plan usually relies on one or more of these tools:
Interproximal reduction
Also called IPR, this method removes a very small amount of enamel between selected teeth to create modest space. It’s controlled reshaping, not drilling out the tooth. This is often useful for mild crowding.
Palatal expansion
This widens the upper arch to create room and improve the fit of the bite. Expansion tends to be more straightforward in younger patients whose growth is still on their side.
Space maintenance
In children, preserving space after early loss of a baby tooth can prevent future crowding from getting worse. It doesn’t replace orthodontics, but it can reduce how complicated treatment becomes later.
Non-extraction braces or aligners
Braces and clear aligners can often align teeth without extraction when crowding is limited and the bite can be corrected within the boundaries of the bone and soft tissue.
A survey covered in this study on extraction trends and alternatives found that 52.5% of orthodontists were unhesitant to extract when clinically needed, while IPR was the most favored non-extraction method at 34.3%. The same source notes that extraction becomes more likely as crowding severity and certain bite patterns increase.
That fits what patients see in real life. If only a small amount of room is needed, IPR or careful arch development may be enough. If the teeth are severely crowded or the bite discrepancy is larger, non-extraction treatment can become a compromise rather than a solution.
| Option | Best for | Limitation |
|---|---|---|
| IPR | Mild space needs | Creates only limited room |
| Expansion | Narrow arches, growing patients | Not every adult case is a good fit |
| Braces or aligners without extraction | Mild to moderate alignment issues | Can push teeth beyond ideal support if overused |
| Extraction | Larger space needs, certain bite corrections | Involves a surgical step and recovery |
A good alternative is not the option that avoids extraction at all costs. It’s the option that solves the actual problem without creating a new one.
If you’re considering aligners, ask whether your case is being designed as a true non-extraction case or a “hope it fits” case. That distinction matters. For patients exploring discreet treatment, clear aligners can be an excellent option when the diagnosis supports them.
Some questions lead to better decisions than others. These are useful:
Patients do best when they stop asking for a yes-or-no answer and start asking for the tradeoffs. Orthodontics is full of tradeoffs. Good care makes them visible.
For many families, the hardest part of treatment planning isn’t the clinical decision. It’s figuring out how to pay for it without feeling cornered.
Orthodontic care can involve several moving parts: records, the orthodontic appliance itself, possible extraction fees, follow-up visits, retainers, and sometimes restorative work later. That doesn’t mean treatment is out of reach. It means you need a clear breakdown before you commit.

A simple extraction case usually costs differently from a complex one because the total picture differs. Factors include the number of teeth involved, how difficult the removal is, whether sedation is needed, and whether you’re doing braces or aligners afterward.
Patients also worry that choosing extraction means sacrificing appearance. That fear can affect financial decisions because people don’t want to pay for a result they may regret. The evidence is more reassuring than online rumor suggests. As noted in the earlier profile discussion, 1 mm of incisor retraction typically produces about a 0.6 to 0.7 mm lip change, which is why careful planning matters so much in facially sensitive cases.
Start with practical questions, not broad ones.
Paying for care is easier when the plan is transparent. Confusion creates more stress than the actual numbers in many cases.
If affordability is a top concern, resources like this guide to affordable dental care in Houston can help you understand common financing and membership-plan approaches before you schedule.
A good office should be able to explain costs in plain language. You shouldn’t have to decode billing terminology while also deciding whether extraction is right for your child or for yourself. Clear treatment planning and clear financial planning belong together.
If you remember one thing from this guide, let it be this: an orthodontist tooth extraction is not a punishment, a shortcut, or an old-fashioned reflex. It’s one treatment option among several. In the right case, it creates the space needed for a healthier bite, better alignment, and a more stable result. In the wrong case, it would be unnecessary. That’s why diagnosis matters more than opinion.
The best treatment decisions usually come from a combination of careful records, honest conversation, and realistic expectations. If a clinician can show you the crowding, explain the bite problem, compare alternatives, and talk clearly about recovery, you’re in a much better position to choose with confidence.
Families in Humble, Atascocita, Kingwood, and the greater Houston area often need more than a one-step answer. They need a place that can look at the full picture, from digital imaging to orthodontic planning to routine dental care and long-term maintenance. They also need communication that doesn’t make the process feel harder than it already is.
That’s what good dental care should feel like. Clear. Respectful. Practical. Personal.
If you’re near 12235 Will Clayton Parkway, Suite #4, Humble, TX 77346, across from Walmart, the next step is simple: schedule a consultation, bring your questions, and ask for the reasoning behind every recommendation. The right plan should make sense to you, not just to the chart.
If you’re ready for answers about crowding, bite issues, clear aligners, extractions, or affordable treatment options, Clayton Dental Studio offers compassionate, complete care for children, teens, and adults in Humble and the greater Houston area. Dr. Navneet Kamboj and the team provide modern diagnostics, patient-first guidance, flexible financing through CareCredit and Cherry, and the Humble Savings Plan for patients without insurance. Call or book online to schedule your consultation and take the next step toward a healthier, more confident smile.