

Book Your Appointment Today!
Our staff will reach out to you shortly
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
You finally decide to replace a missing tooth. You’re ready for the implant, you’ve pictured the finished smile, and then you hear something that feels like a setback: “There isn’t enough bone there yet.”
That moment catches a lot of people off guard. They assume the missing tooth is the problem, but the underlying issue is often the support underneath it. Teeth sit in jawbone, and when a tooth has been missing for a while, the bone in that area can shrink.
That’s where bone grafting services come in. A bone graft isn’t a detour from treatment. It’s often the step that makes treatment possible. For many patients, it’s the bridge between “not yet” and “yes, you can get that implant.”
You come in ready to talk about replacing a missing tooth. Then the exam shows something you were not expecting. The space is there, but the support underneath it is not as strong as it needs to be.
That can feel discouraging at first. In reality, it is often a sign that your dentist is looking past the immediate fix and planning for a result that can stay stable for years.
Your jawbone works like the soil around a fence post. If the ground has worn away, the post may still go in, but it is less likely to stay firm under pressure. A dental implant needs that same kind of steady support. When bone has become too thin or too soft, a bone graft can rebuild the area so the next step has a better base.
Patients often worry that hearing "you need a graft" means the situation is severe or unusual. It usually means the opposite. Bone grafting is a familiar part of modern dental care, especially for people preparing for implants or trying to preserve the shape of the jaw after tooth loss.
Comfort matters here too. Many people are less anxious once they understand that bone grafting is planned carefully, done with numbing and comfort options, and mapped out with imaging that shows the area in detail before treatment starts. Clear planning helps reduce surprises, and fewer surprises usually means less stress.
A bone graft usually means your dentist is creating better conditions for the final result, not reacting to a failure.
It also helps to know what happens after this recommendation. You should expect a straightforward conversation about why the graft is needed, how much bone support is missing, what type of graft may fit your case, how healing fits into the timeline, and what the costs may look like at each stage. For a nervous patient, that kind of transparency can be very reassuring.
The goal is simple. Give your future smile a stronger foundation, make the process feel more predictable, and help you understand each step before anything begins.
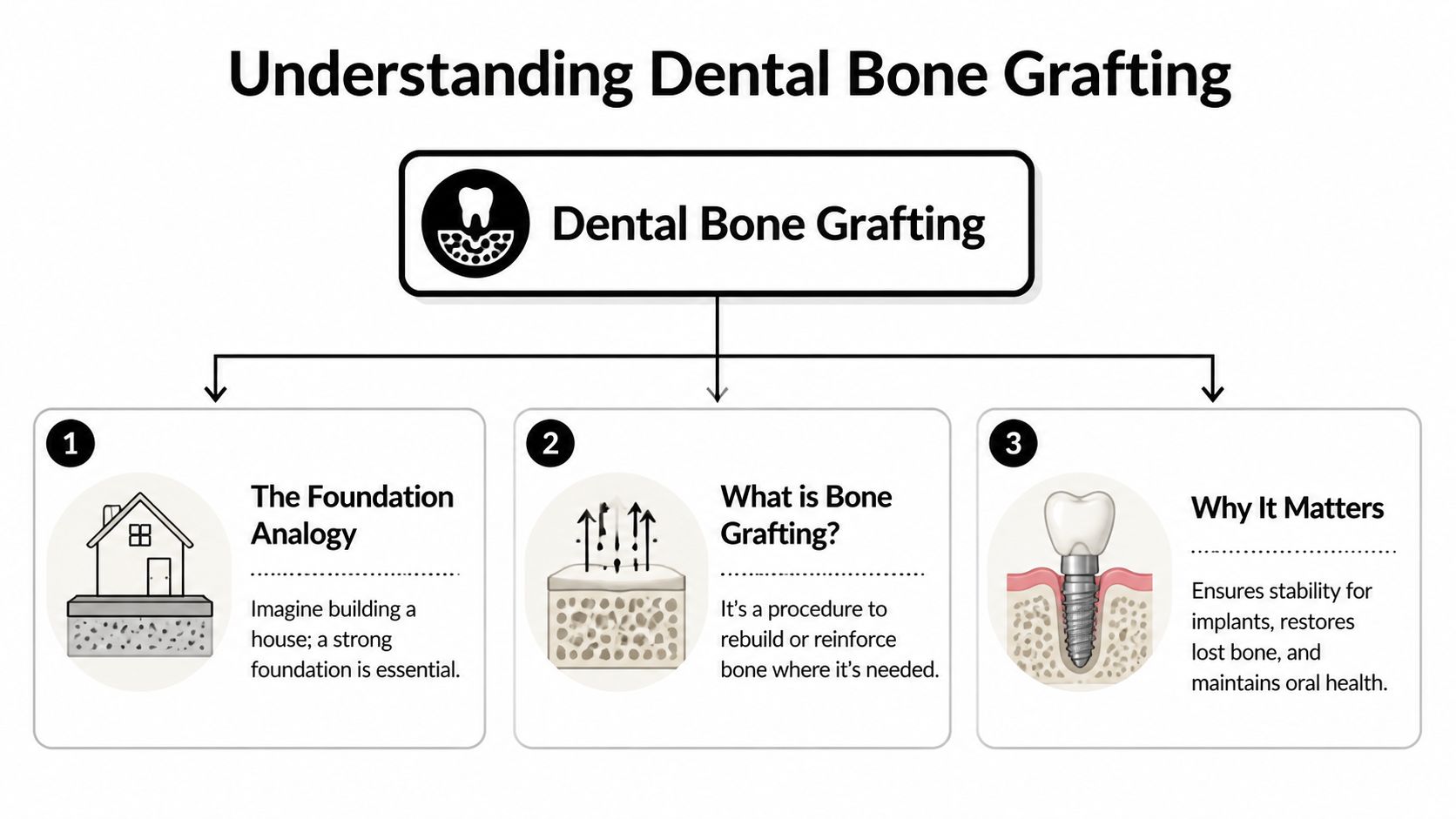
Bone grafting is easier to understand if you think like a builder. Before putting up a house, you need solid ground and a stable slab. If the foundation is weak, everything above it is at risk. In dentistry, the jawbone is that foundation.
A dental bone graft is a procedure that adds material to an area where bone has been lost or where extra support is needed. Over time, your body uses that material as a scaffold and begins building new bone in that space. The goal is simple: create enough healthy bone to support a future implant or preserve the shape of the jaw after a tooth is removed.
Patients generally don't require an extensive biology lesson. They want to know why this step matters. The answer is that bone supports both function and appearance.
Without enough bone, a future implant may not have the strength it needs. Bone loss can also change how the gumline looks and how the face is supported in that area. Rebuilding bone helps protect the long-term plan, not just the next appointment.
Here’s the plain-language version of what a graft can help with:
Patients often ask, “What exactly are you putting in there?” That’s a good question. Dentists choose from a few main categories, and each one has a different reason for being used.
| Graft type | What it means in plain language | Why it may be chosen |
|---|---|---|
| Autograft | Bone taken from your own body | It contains your own cells and growth factors |
| Allograft | Processed donor bone | It avoids a second surgical harvest site |
| Xenograft | Bone material from an animal source, commonly bovine | It serves as a framework for new bone growth |
| Alloplast | Synthetic graft material | It offers a manufactured option with predictable handling |
An autograft is often considered the gold standard because it comes from you. According to Cleveland Clinic’s bone grafting overview, autografts contain the patient’s own cells and growth factors, minimize immune rejection, and have shown fusion success rates exceeding 95% within 6-12 months.
That doesn’t mean every patient needs an autograft. In routine dental care, many dentists also use donor, animal-derived, or synthetic materials very successfully. The choice depends on the size of the defect, the treatment goal, your health history, and whether the site needs volume, structure, or a material that holds space well.
Practical rule: The “best” graft isn’t one material for everyone. It’s the one that fits the exact site, your treatment goal, and your comfort level.
This is also where confusion tends to start. Some patients think graft material acts like a permanent filler. Usually, the point is different. The material helps guide or support your body’s own healing so the area becomes more suitable for future function.
A dentist chooses a bone graft the same way a builder chooses a repair method. The plan depends on what is missing, what needs support, and what the area needs to do later. For one patient, the goal is to protect the bone right after an extraction. For another, it is to rebuild bone that has slowly thinned over time. In the upper back jaw, the challenge is often limited space because the sinus sits close to the tooth roots.

After a tooth is removed, the empty socket begins to heal and reshape. That process is normal, but it can also reduce the bone volume that would support a future replacement tooth.
A socket preservation graft is placed into the socket soon after the extraction. Its job is to help the area keep its shape while your body lays down new bone. A simple way to understand it is to picture the socket as wet soil after a post is removed. If nothing supports the space, the walls can slump inward as healing progresses.
This option often makes sense for patients who are not getting an implant the same day but want to keep that option open later. It can also help the final replacement look more natural because the gumline and ridge contour are better supported.
If a tooth has been missing for months or years, the jaw in that spot can lose width, height, or both. You may hear the term “collapsed ridge.” It means the bone no longer has the shape needed for strong, well-positioned tooth support.
A ridge augmentation graft rebuilds that lost volume. Some areas need a wider ridge so an implant can sit securely. Other areas need more height to create enough support for chewing forces and a natural-looking result. In many cases, both function and appearance matter.
Patients exploring dental implant options in Humble are often surprised to learn that the visible tooth is only part of the plan. The bone underneath is the foundation. If the foundation is too thin, the final result can be harder to place in the right position and harder to maintain over time.
The upper back jaw has a unique design. Above the molars and premolars sits the sinus cavity, which can leave limited bone height for an implant after bone loss or long-term tooth absence.
A sinus lift creates more room for bone in that area by gently lifting the sinus membrane and placing graft material below it. The goal is straightforward. It increases the amount of bone available so a future implant has better support.
The name can sound intimidating. For many patients, the anxiety comes more from the word “sinus” than from the procedure itself. In practice, it is a targeted solution for a specific anatomy problem, and careful imaging helps the dentist decide whether it is needed at all.
The easiest way to sort these procedures is to ask what problem the graft is solving.
| Situation | Common grafting approach | Main purpose |
|---|---|---|
| Tooth is being removed now | Socket preservation | Maintain the shape of the site |
| Tooth has been missing and bone has shrunk | Ridge augmentation | Rebuild width or height |
| Upper back jaw lacks enough vertical bone | Sinus lift | Add bone beneath the sinus area |
If your dentist recommends grafting, ask this question: “Are we protecting the bone I still have, or rebuilding bone that is already gone?” That one answer often makes the treatment plan feel much clearer, and it gives you a better sense of what happens next, how long healing may take, and why the recommended option fits your case.
What calms anxiety most is knowing what happens next. Bone grafting feels less overwhelming when you can picture the process from the first visit through healing at home.

Your first visit usually starts with imaging, an exam, and a conversation about goals. If you’re hoping for an implant, the key question is whether the area has enough bone now or needs help first.
Modern imaging proves invaluable. A three-dimensional scan gives the dentist a more complete look at width, height, and nearby structures than a basic two-dimensional image alone. Patients who want to understand this part better can review CBCT imaging technology in Humble, which shows how detailed scans support planning.
The planning visit is also when you should bring up concerns that feel small but matter a lot. Are you nervous about pain? Do you have a tight work schedule? Are you trying to understand timing before a wedding or a family event? Those details shape the treatment plan.
Most bone grafting procedures in general practice are done with local anesthesia so the area is numb. Some patients also discuss sedation options if dental visits make them especially uneasy. During the procedure, the dentist prepares the site, places the graft material, and protects it so healing can begin undisturbed.
What patients usually notice most is pressure, not sharp pain. You may hear sounds or feel movement, but the goal is a controlled, comfortable appointment. If the graft is done at the time of an extraction, the sequence often feels more straightforward than people expect.
A short visual overview can make that easier to picture:
After the graft is placed, your body takes over. Over time, the site matures and becomes more suitable for the next phase of treatment. This part requires patience because healing isn’t just about the gum surface looking better. The deeper bone changes matter most.
Patients often ask whether they’ll feel the graft “working.” Usually, no. Healing is gradual and mostly invisible. Your dentist monitors progress with follow-up visits and imaging as needed.
The home-care phase matters more than many people realize. The first days are about protecting the site and letting the blood clot and soft tissues settle.
A few practical habits help most patients:
Healing is usually smoother when patients protect the site instead of checking on it repeatedly. In bone grafting, “leaving it alone” is often good care.
You may be at the point where the plan sounds clear, but one question still lingers. Is bone grafting really worth doing?
That question deserves a straight answer. A graft is not an extra step added for convenience. It is often the way a weak or shrunken area of jawbone is built back up so it can support the tooth replacement you want. If an implant is like a post in the ground, the bone is the soil holding it steady. Without enough healthy bone, the final result may be harder to place well, harder to keep clean, or less predictable over time.
Many people choose bone grafting because it improves the foundation before the visible part of treatment begins. That can matter if you want an implant, want to preserve the shape of your jaw after tooth loss, or want the final tooth to sit in a position that looks and functions more naturally.
Patients sometimes worry that needing a graft means their case is somehow second-rate. It usually means the dentist is addressing the problem properly instead of forcing an implant into a site that is not ready for it. As noted earlier, implants placed after grafting can still perform very well when the case is planned carefully and healing is monitored properly.
There is also a long-term benefit that is easy to miss in the beginning. Better bone support can give your restorative dentist more control over where the implant goes, which can affect your bite, the appearance of the gumline, and how easy the area is to maintain years from now.
Every surgical procedure has tradeoffs, and bone grafting is no exception. Possible risks include infection, delayed healing, irritation at the site, loss of some graft material, or needing more healing time before the next phase.
One term that often causes confusion is resorption. This means your body gradually replaces some of the graft as it heals. That is not automatically a problem. In fact, some amount of change is expected. The important consideration is whether enough strong, stable bone remains for the final goal.
That is why the discussion should be specific to your case. A small socket graft after an extraction is different from a larger augmentation in an area that has been missing a tooth for years. Good planning includes explaining what could happen, how healing will be checked, and what the backup plan is if the site needs more time.
Cost can feel like the most stressful part because it is rarely one flat number. The total fee may depend on the size of the graft, the material used, imaging, whether the graft is done at the same visit as an extraction, and whether implant treatment is part of the larger plan.
Ask for the estimate in pieces. That makes it easier to see what you are paying for now, what may come later, and which parts might involve insurance or financing. A written breakdown of diagnosis, grafting, follow-up visits, and future restoration costs can reduce the kind of uncertainty that makes people delay care.
If insurance is involved, pre-treatment coordination can help limit surprises. Some dental teams also use administrative tools to enhance patient care with AI authorization so approvals and documentation are handled more efficiently behind the scenes.
If the numbers still feel overwhelming, payment options matter. Financing plans, phased treatment, and in-house membership programs can make care more manageable, and this guide on how to afford dental work explains common ways patients spread out dental costs.
A good decision usually comes back to four questions:
Bone grafting often makes sense when it improves the odds of a result that feels stable, comfortable, and worth keeping for the long term.
You might hear the words "bone graft" and picture a long, uncomfortable process with a lot of unknowns. A good treatment experience feels much more grounded than that. It starts with understanding why the bone needs support, what the plan is, and what each step is meant to accomplish.
Bone grafting works best when the site is mapped carefully before any treatment begins. Digital imaging lets the dentist study the shape of the bone, the amount of space available, and the location of nearby structures. That matters because a graft is not one-size-fits-all. It is closer to repairing the foundation under a house. The repair has to match the space it is supporting.
This early planning also helps answer a question many patients have right away: "Do I really need this?" In some cases, the goal is to preserve the area after an extraction. In others, it is to build enough support for a future implant or to improve the contour of the ridge for a more stable result. When patients can see the area on a screen and hear the reason in plain language, the recommendation usually feels less mysterious.
The clinical side is only part of the experience. Anxiety often comes from uncertainty, not from the procedure itself.
Clear explanations, local anesthesia, and a calm pace can make bone grafting feel far more manageable. Many patients are relieved to learn that the appointment is usually about staying numb, comfortable, and informed while the area is treated carefully. A well-organized office also helps. It signals preparation, consistency, and attention to detail, which can lower stress before a word is spoken.
For patients in Humble, Atascocita, Kingwood, and the greater Houston area, Clayton Dental Studio is one option for bone grafting services connected to implant planning, restorative treatment, digital imaging, and financing support in one setting. That can make the process feel simpler because the diagnosis, treatment planning, and next steps are easier to follow when they are coordinated together.
Communication plays a big role here. Patients usually want more than a technical answer. They want to know what will happen, how recovery may feel, how long healing may take, and what costs may show up now versus later. If you are interested in how dental practices present complex care in a patient-friendly way, Bruce & Eddy's dental marketing insights offer an interesting look at how offices explain treatment clearly enough for patients to make informed decisions.
A few questions can make the whole process feel clearer:
Patients facing bone grafting usually do better when the process is explained like a journey, not a single procedure. The goal is simple. You should know why the graft is being recommended, how your comfort will be protected, and what happens after the area heals.
Most patients do well with local anesthesia, so the procedure itself is usually more about pressure than pain. It’s normal to have soreness afterward, especially for the first few days, but discomfort is typically managed with the instructions and medications your dentist recommends.
That depends on the type of graft, the size of the area, and how your body heals. Some cases move to implant placement after a healing period, while others require more time before the bone is ready. Your dentist should give you a timeline based on your specific site rather than a generic estimate.
It can come from your own body, donor tissue, an animal-derived source, or a synthetic material. The right choice depends on the treatment goal and your anatomy. If you’re unsure, ask your dentist to explain why that material was chosen for your case instead of naming the category.
Coverage varies. Some plans may help with portions of diagnosis, extraction-related procedures, or medically necessary parts of treatment, while others may not contribute much toward implant-related care. The safest step is to ask for a pre-treatment estimate and a written financial breakdown before scheduling.
The goal usually isn’t for the graft to remain unchanged forever. In many cases, the material acts as a scaffold while your body heals and remodels the area. Your dentist is planning for that process, not expecting the site to remain static.
Resorption means the body naturally breaks down some of the graft during healing. That’s part of why case selection and technique matter. According to this discussion of graft stability and onlay resorption, onlay grafts for jaw augmentation can experience 10-30% resorption, which is one reason dentists pay close attention to material choice and long-term support in larger cases.
That’s common. Ask your dentist to walk you through the appointment in simple terms: how the area will be numbed, what you’ll feel, what you’ll eat afterward, and when you’ll be checked again. Anxiety often drops when the process stops feeling vague.
If you’re considering an implant or you’ve been told you don’t have enough bone yet, a consultation can give you a clear next step. Clayton Dental Studio provides modern imaging, restorative planning, and transparent guidance so you can understand your options and decide what feels right for your smile.