
Book Your Appointment Today!
Our staff will reach out to you shortly
Thank you! Your submission has been received!
Oops! Something went wrong while submitting the form.
If you’re searching for “overdenture near me”, you’re probably dealing with one of two situations. Either your current denture moves when you talk and eat, or you’ve been told you need a full-arch tooth replacement and want something steadier than a traditional plate.
I hear the same worries in consultations all the time. Patients want to know whether they’ll still need adhesive, whether they’ll be able to chew comfortably, whether the process is painful, and whether implants are even realistic if they’ve already lost bone or have a medical condition like diabetes.
An overdenture can be a very practical middle ground. It isn’t the same as a loose conventional denture, and it isn’t the same as a permanently fixed bridge either. It’s a removable denture that connects to implants for added grip and control. For many people, that changes daily life in simple but meaningful ways. Meals feel less stressful. Speech feels more natural. Social situations stop feeling like a test.
A traditional denture is a bit like a boat resting on water. It can work, but it can also drift. An overdenture is more like that same boat with anchors in place. The denture still comes out for cleaning, but it has stable points that help hold it where it belongs.

The foundation is the implant. A dentist places small implants into the jawbone, and those implants act like anchors. The overdenture then connects to those anchors through a special attachment system.
That connection is the part patients usually notice most. With a regular denture, the denture mostly rests on the gums. With an overdenture, the implants help control movement. That can reduce slipping, rocking, and the little shifts that make people nervous when they laugh or chew.
Overdentures are still removable. That’s important. Many patients want better stability but also want something they can take out at home to clean. This design gives both.
The need for stable tooth replacement is large. Data cited in these denture statistics notes that 99 million people in the U.S. wore dentures in 2020, and the same source projects 42.46 million Americans will use dentures by 2025. It also states that over 30% of adults aged 65+ in high-income countries are completely toothless. Those numbers help explain why so many families are looking for more secure denture solutions.
Simple rule: If your main complaint is movement, an overdenture is designed to address movement.
Patients usually care less about the technical term and more about the daily result. They want to know what changes at breakfast, during conversations, and in photos.
Here’s the plain-language version:
Some patients also compare it with bridges, partials, or fixed implant options before deciding. If you’re weighing those choices, this guide to best options for missing teeth can help you sort out which category fits your needs.
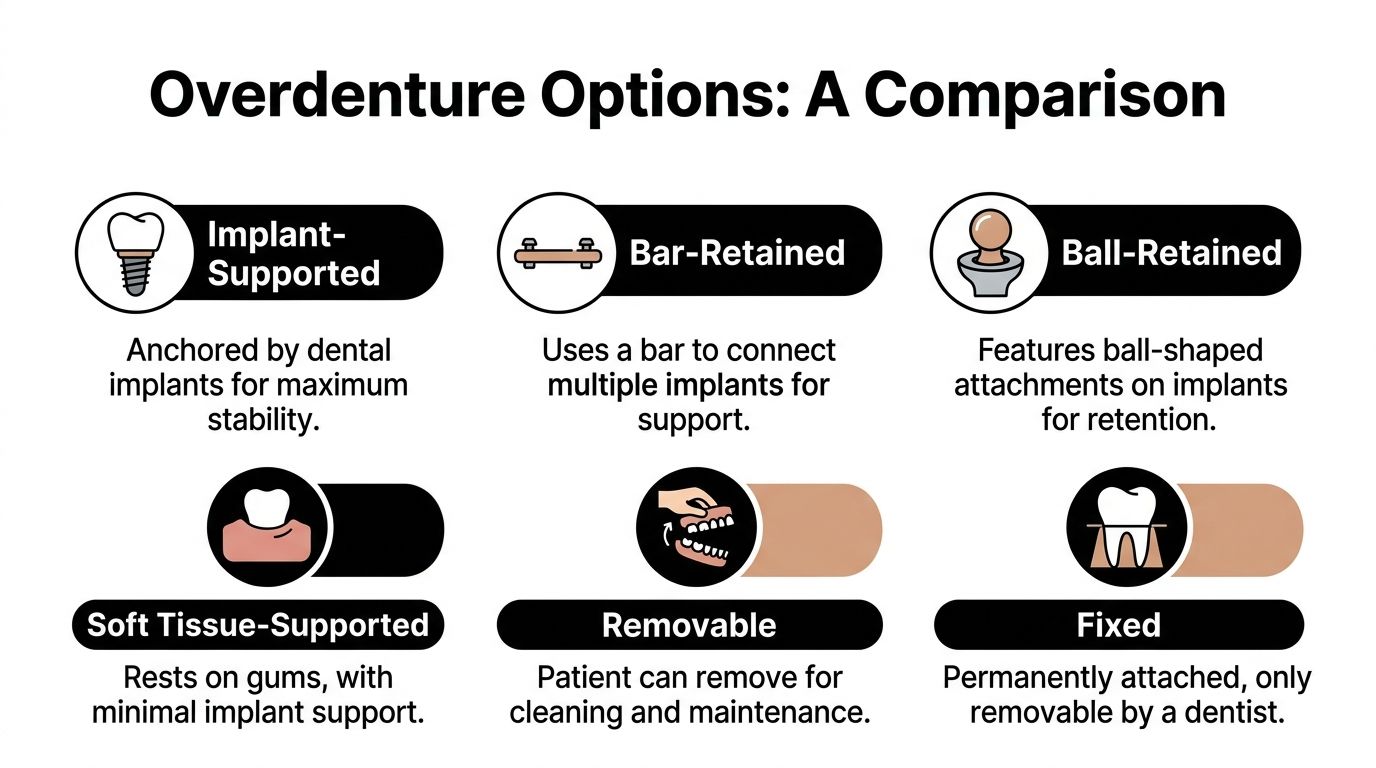
Not all overdentures work the same way. Two patients can both say they want a “snap-in denture” and still need very different designs.
One person may need a denture that gets most of its support from the gums and uses implants mainly for retention. Another may need a design where implants do more of the support work. Then there’s the attachment system itself, which affects feel, maintenance, and how the denture goes in and out.
These phrases sound similar, so patients often assume they mean the same thing. They don’t.
Implant-retained overdentures use implants mainly to help the denture stay in place. The denture may still rely partly on the gum tissue for support. For many people, this is a practical way to improve stability without moving into a more complex full fixed restoration.
Implant-supported overdentures shift more of the workload to the implants themselves. That can mean a firmer feel and less pressure on the gums, depending on the case and design.
Neither one is automatically “right” for everyone. The right choice depends on your bone, bite, dexterity, expectations, and budget.
Most consultations eventually come down to this question: what will hold the denture onto the implants?
A common option is the locator-style attachment, often described by patients as a snap-on system. Another is a bar attachment, where multiple implants are connected by a bar and the denture engages that bar.
Modern systems have expanded what’s possible. According to the LOCATOR Overdenture System manual, narrow-diameter implants can be as small as 2.4 mm, and the attachment design can accommodate up to 40 degrees of divergence between implants. In plain language, that means some people with irregular or reduced bone still have options.
When bone shape isn’t ideal, the plan doesn’t always end there. The attachment system matters more than many patients realize.
| Feature | Locator (Ball) Attachments | Bar Attachments |
|---|---|---|
| How it works | Denture snaps onto individual implant attachments | Denture connects to a bar joining implants |
| Feel | Secure, with a simple in-and-out motion for many patients | Often feels more unified and stable |
| Cleaning | Usually straightforward to remove and clean | Can require more detailed cleaning around the bar |
| Maintenance | Retentive parts may wear and need replacement over time | Bar and clip maintenance depends on fit and hygiene |
| Bone challenges | Often useful when planning around implant angulation limits | Can help distribute forces across connected implants |
| Who may like it | Patients who want simplicity and removability | Patients seeking a stronger connected framework |
Locator-style systems are often easier for patients to understand because each implant acts like an individual snap. Bar systems can feel more engineered because the implants work together through one connected structure.
That doesn’t make one universally better. It changes the conversation.
A patient with reduced hand strength may value a simpler removal routine. Another patient may care most about a more rigid feel. Someone with challenging bone anatomy may need a treatment plan shaped around implant position first, then the attachment choice follows.
If you’re looking locally at removable implant options, this page on implant retained dentures in Humble shows the kind of treatment category many patients mean when they search for “overdenture near me.”
The first question patients ask is straightforward. “Will this work for me?”
That answer depends on your mouth, your health, and your goals. A person can be an excellent candidate even if they’ve worn dentures for years. Another person may need medical coordination or pretreatment before implants are placed.

Many patients assume they’ve waited too long. They think bone loss automatically disqualifies them. That isn’t always true.
Some implant systems are designed for tighter spaces and more complex anatomy. Treatment planning starts with imaging and a close look at where bone remains, not with guesswork. Even when the ridge has changed over time, there may still be a workable path.
What matters is not just “do you have bone,” but whether the available bone can support a safe, thoughtful design.
A consultation for overdentures should include more than teeth and gums. It should cover medications, healing history, chronic health conditions, and how well those conditions are controlled.
One of the most important examples is diabetes. As noted by this discussion of denture candidacy and diabetes, patients with uncontrolled diabetes may face a 14% implant failure rate compared with 7% in non-diabetics. That doesn’t mean diabetics can’t get overdentures. It means the condition needs to be taken seriously, and blood sugar control should be part of treatment planning.
Clinical point: Controlled health conditions are very different from uncontrolled ones. The question isn’t just what diagnosis you have. The question is how stable it is today.
Other factors also shape candidacy:
A proper workup often looks at several layers at once:
For a visual overview of how dentists assess fit, support, and treatment planning, this video gives helpful background:
Some of the most grateful overdenture patients are people who’ve struggled with loose dentures for years, have moderate bone loss, or need a removable option they can maintain more easily than a fixed full-arch bridge.
The key is matching the treatment to the person. If you’re medically complex, that doesn’t end the conversation. It means your planning needs to be more careful.
Understanding the process in steps provides comfort. Overdentures don’t happen in one sitting for most patients, and that’s a good thing. Each phase has a purpose.
The first visit is usually a diagnostic visit. The dentist examines your mouth, reviews your medical history, checks your existing denture if you have one, and studies imaging to see where implants could go.
This is also when expectations get clarified. Some patients want the smallest number of implants needed to reduce movement. Others want the most stable removable option possible. Those are different goals, and the plan should reflect that.
Once the plan is set, the implants are placed in the jaw. The procedure itself is more controlled and methodical than many patients expect.
Your comfort options are discussed in advance. Some people do well with local anesthesia alone. Others prefer additional support for anxiety. The exact experience depends on the scope of treatment and your comfort needs.
Most patients are relieved to learn that implant surgery is usually less dramatic than they pictured.
After placement, the bone needs time to heal around the implants. This is the phase where the implants become stable enough to support the overdenture attachments.
During healing, you may wear a temporary denture or a modified version of your current denture. The dentist gives instructions about diet, cleaning, and how much pressure to place on the area while things settle.
Healing time varies from case to case. Bone quality, general health, whether teeth had to be removed, and whether any additional procedures were needed all affect the timeline.
Once the implants are ready, the restorative phase begins. This includes impressions or digital records, bite registration, tooth setup decisions, and attachment selection.
Several details are checked carefully:
A good overdenture should not only stay in better. It should also look natural and feel manageable to use.
The delivery appointment is not the end of treatment. It’s the start of the maintenance phase.
Small bite adjustments are common. So are conversations about cleaning routines, nighttime habits, and what degree of tightness feels comfortable. Some patients need a little time to learn the insertion path, especially with new attachments.
That’s normal. It’s comparable to getting used to a new pair of glasses. The benefit is real, but there’s a short adaptation period while your muscles and habits catch up.
Cost matters. It matters a lot. Patients don’t need vague answers here. They need a realistic framework for what they’re paying for and what they’re getting in return.

According to this overview of dentures and overdentures, overdentures typically cost $10,000 to $20,000 per arch, while traditional dentures often range from $1,500 to $3,000. That difference is significant, and patients are right to ask whether the added investment is worth it.
The reason for the higher cost is simple. You’re not paying only for the denture. You’re paying for surgery, implant components, attachment parts, planning, fabrication, and follow-up.
The same source notes that overdentures can reduce future jawbone loss by up to 75% and show 10-year survival rates of 80% to 90%. Those are not small differences. They matter because tooth replacement isn’t only about having teeth in a photo. It’s about function, facial support, and how much retreatment you may need later.
When the jawbone continues to shrink, dentures tend to get looser. That can mean more adjustments, more frustration, and more compromise in comfort over time. Overdentures address that issue more directly because the implants help stimulate and preserve the bone.
Value test: If a treatment helps you chew better, keeps the denture steadier, and supports the jaw over time, the cheapest option may not be the least expensive one in the long run.
No two estimates are identical. Several things push the number up or down:
An overdenture is not a one-time purchase that you ignore forever. Attachments wear. Tissue changes. Bites shift. Regular maintenance protects the implants and keeps the denture functioning the way it should.
That’s another reason I encourage patients to compare not just sticker price, but the full picture. Ask how often follow-up is expected. Ask what parts may eventually need replacement. Ask how cleaning should be done at home. Good value comes from durability plus maintainability.
If financing is part of your decision, resources like this guide to affordable dental implants in Houston can help you think through budgeting and payment options before your consultation.
You may be sitting at your kitchen table with a loose denture in one hand and your phone in the other, searching for “overdenture near me” because eating, speaking, and smiling have started to feel unpredictable. In that moment, the right office is not just the closest one. It is the one that can explain your options clearly, check whether your health history changes the plan, and help you understand what will keep your jawbone and implants healthy for years.
That broader view matters. The U.S. overdenture and implant bridge market continues to grow, which reflects how common implant-supported tooth replacement has become. Growth alone does not tell you which practice is careful, though. A good consultation should connect the mechanics of the denture, the biology of bone support, and the realities of your medical history.
An overdenture works a bit like a house built on a stable foundation. The visible part is the denture, but long-term comfort depends on what supports it underneath. That is why I tell patients to look beyond the phrase “snap-in teeth.” Ask whether the office discusses bone preservation, attachment maintenance, and the difference between a plan that merely holds better today and one that is designed to serve you well over time.
Medical conditions matter here too. Patients with diabetes, a history of gum disease, dry mouth, or slow healing often need more careful planning, not automatic exclusion. The key is thoughtful evaluation, good home care, and follow-up that catches small problems early.
At Clayton Dental Studio, Dr. Navneet Kamboj and the team provide family and restorative dental care in one location, including denture-related treatment planning, implant-retained denture options, digital AI-powered X-rays, and financing pathways such as CareCredit, Cherry, and the Humble Savings Plan. For many patients, that matters because overdentures are not a one-visit treatment. They involve diagnosis, planning, healing, fitting, and maintenance.
The office is located at 12235 Will Clayton Parkway, Suite #4, Humble, TX 77346, across the neighborhood from Walmart. Patients in Humble, Atascocita, Kingwood, and nearby Houston communities often want care close to home because overdenture treatment usually includes several visits over time.
When you call, ask questions that reveal how the office thinks:
Patients who want to understand why some nearby healthcare offices are easier to find and compare online can read this guide on Local SEO for medical practices. It helps explain how location details, services, and patient-focused information are presented online.
Take it out as directed, clean the denture gently, and clean around the implant attachments carefully. The key is that you’re maintaining both the denture and the tissue around the implants.
Use the tools your dentist recommends. Don’t improvise with harsh products or abrasive pastes. The goal is thorough cleaning without damaging attachment components.
In many cases, yes. Some patients have one arch treated first and the other later. Others are candidates for both arches, depending on bone, bite, and treatment goals.
The upper jaw and lower jaw don’t always behave the same way, so the design may differ from one arch to the other. That’s normal.
It depends on when it happens and how the denture was designed. Sometimes the failed implant can be replaced after healing. Sometimes the denture can be modified temporarily while a new plan is made.
The important point is not to ignore symptoms. If an overdenture starts feeling different, looser, or sore in one area, get it checked promptly.
If something suddenly changes with fit or comfort, don’t “wait it out” for months. Small issues are easier to manage early.
No. They’re common in older adults, but they’re not limited to seniors. Younger adults with significant tooth loss, failing teeth, or complex restorative needs may also be candidates.
The better question is whether a removable implant-supported solution fits your life better than a fixed bridge, a conventional denture, or another form of restoration.
Usually, it feels better quickly, but “natural” is a process. Your lips, cheeks, tongue, and chewing muscles need time to adjust to any new prosthesis.
Most patients improve steadily as they learn the insertion path, chewing rhythm, and cleaning routine. A few follow-up visits often make a big difference.
For many people, yes, especially if they want more stability than a conventional denture but aren’t ready for a fixed full-arch solution. It still requires a meaningful investment, though, so the right plan depends on your priorities.
Some patients decide that removability, easier cleaning, and lower cost than a fully fixed restoration make overdentures the most sensible compromise.
If you’re weighing your options and want a clear, pressure-free conversation, Clayton Dental Studio can help you understand whether an overdenture fits your health, your goals, and your budget. A consultation is the best place to review bone support, medical factors, denture stability, and financing options so you can make a confident decision.